
By Briahnna Brown
About one third of people hospitalized from COVID-19 in March were African American, according to recent data from the Centers from Disease Control, despite making up only 18 percent of the population in the U.S. areas studied.
While the available data offers only a glimpse at the developing situation, the apparent racial and economic disparities are significant. Wendy Ellis, Dr.P.H. ’19, director of the Building Community Resilience Collaborative and Networks at the George Washington University Milken Institute School of Public Health, has designed and implemented a strategic approach aimed at understanding and addressing these disparities.
The disparities that the COVID-19 pandemic have brought to light are not a result of the virus but a reflection of systemic issues in the United States, Dr. Ellis said. She spoke with GW Today to explain how these health disparities have come to light:
Q: What are the health disparities that the COVID-19 pandemic has brought to light?
A: The disproportionate impact of COVID-19 can be measured along the country’s race and poverty lines. As illustrated by the growing number of COVID-19-related fatalities in individuals with pre-existing conditions, such as diabetes, obesity, heart disease and asthma, the virus exploits a long-standing disproportionality in the burden of chronic disease and shortened life expectancy that follows a racial and income gradient. Those at the lower end of the economic spectrum bear a higher burden of chronic disease, a burden that makes them more susceptible to severe illness associated with COVID-19.
Q: What drives the health disparities along race and poverty lines?
A: The negative health outcomes we see today are the result of the concentration of poverty and lack of access to supports and buffers that promote health and economic security. Public policy enacted nationally and in communities across the country established patterns of poverty, limiting access to quality education and affordable health care.
These policies, implemented over the past 400 years, were designed with either the explicit intent of racial oppression or willfully ignorant of disparate impacts. For example, during the New Deal, federal mortgages were only available to families purchasing a home in “whites only” neighborhoods. As a result, entire swaths of American cities became redlined—meaning banks would not underwrite mortgages or invest. Nearly 70 years after this practice first began, the patterns of race- and place-based outcomes follow these redline maps, where we can see the concentration of poverty, the least resourced schools and the largest food deserts—all contributors to the burden of chronic disease. These are natural outcomes of policy and system design intended to limit access to health, well-being and prosperity for communities of color and the poor.
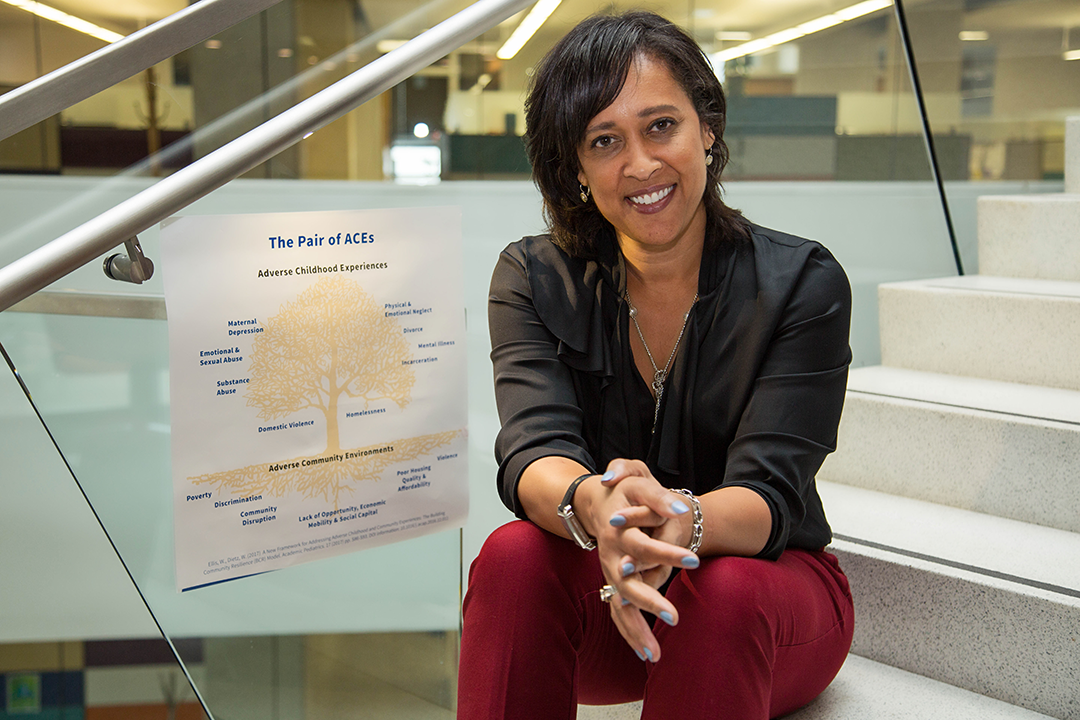
At the Center for Community Resilience, we think about adversity at both the individual and community level through the lens of the Pair of ACEs: a tree planted in soil steeped in systemic inequities, robbing it of nutrients necessary to support a thriving community. If adverse community environments are the roots of inequity and adverse childhood experiences are the fruit of the tree, inequitable policies are the elements in soil that rob the community of vital nutrients, sustaining inequity. Asking, “What’s in your soil?” gets to root causes of trauma and despair.
In our current world of COVID-19 response, these systemic and systematic inequities are creating negative outcomes for vulnerable communities lacking access to supports and buffers.
Q: How do these disparities impact the essential workforce?
A: Many essential workers, including grocery store employees, sanitation workers and transportation workers, reside in low-income communities and do not have the privilege of working from home or practicing physical distancing. It is ironic that our lowest paid workers—those with the least amount of workplace and financial protections—are finally being recognized as “essential,” bearing the highest risk for the lowest return.
As an example, home health aides—a workforce tending to patients who are at higher risk of severe illness from COVID-19—struggle to find the personal protection equipment necessary to protect themselves and their patients. As the pandemic stretches on, we hear each day of new stories of the lives lost in the ranks of those deemed essential—bus and subway drivers, school teachers, grocery store clerks, maintenance workers—who felt compelled to report for duty lest they lose hourly wages.
While the pandemic has deemed these workers essential, our failure to invest equitably in communities has put their lives and the well-being of their families at risk.
Q: Is there anything being done to address these disparities during the pandemic?
A: In communities across the country, organizations and stakeholders are attempting to increase access to supports and buffers that promote health and wellbeing for those hardest-hit by the virus. Many public health and governmental leaders are sharing more data on the disparate impact of COVID-19. The ability to track reliable and complete information about health outcomes is a positive first step to addressing the underlying disparities.
Here in Washington, D.C., Martha’s Table in Ward 8 is providing nearly 800 bags of groceries daily to families in need. In Dallas, local libraries have been lending hotspots to schoolchildren to increase access to high-speed internet and facilitate on-line learning while schools are closed. Other efforts to address disparities include widening access to mental and behavioral health via telemedicine and providing flexibility for virtual home visits from school nurses, counselors and those participating in other social service programs. These new innovations to meet families and children where they are during this pandemic and fill critical educational and emotional needs should be part of our normal practice—not just in crisis.
Q: What can people do to address or resolve these disparities?
A: The fundamental ingredient to address disparities is to provide communities with equitable access to resources that support resilience and well-being. Resilience in the face of disparity is not simply a reflection of individual durability, but, as the COVID-19 pandemic demonstrates, derives from the ability to access resources that buffer individuals in times of acute shocks (such as economic stability) and support optimal health and well-being (access to primary care, educational attainment and social connectedness).
We encourage advocates to identify levers and opportunities to promote policy and systems change that align with the following principles of Building Community Resilience:
- Focus on primary prevention of the Pair of ACEs in public health and across systems
- Support trauma-informed transformations within systems and organizations
- Address and eliminate systemic and historic drivers of inequity
- Be grounded in the science of adverse childhood experiences
- Incorporate whole-family approaches in service delivery
- Facilitate and invest in cross-system collaboration and integration
- Be actively anti-racist
